cervical muscles for control of
excessive athetosis.
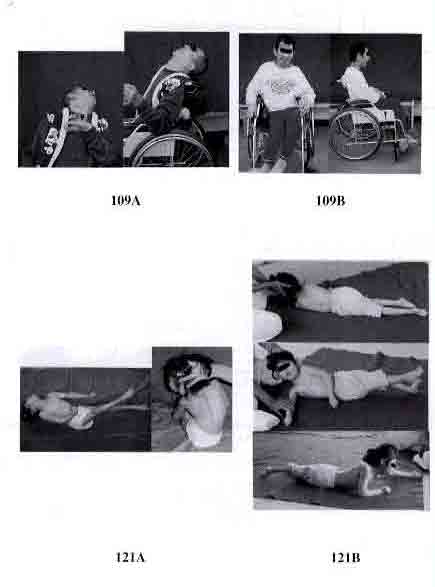
109A: A 47-year-old male
Athetosis quadriplegia,
Involuntary movement due to
athetosis was observed. He
complained of radiating pain,
sensory loss and paralysis of the
upper and lower extremities,
difficulty in fine upper limb
movement and urinary
incontinence.
109B: Postoperatively, radiating
pain, sensory loss and
urinaryand fecal incontinence
were lessened.
Fig.121: Facilitation of turnover
activity by controlling spasticity
of erector spinae muscle
121A: 3-year-old girl,
Spastic quadriplegia
Tonic labyrinthine reflex and
asymmetric tonic neck reflex are
dominant. Spastic scoliosis is
exaggerated when she was held in
sitting posture. There was
difficulty in practicing turnover,
crawling and sitting exercises,
because of excessive spasticity in
the trunk and extremities.
121B: After OSSCS for scoliosis
Top: Scoliosis was corrected.
Middle: Facilitation techniques for
turnover can be effectively
applied.
Bottom: She began to raise and keep
her head upright.
The multiarticular muscles which have less antigravity activity are hyperactive in cerebral
palsy. Therefore spasticity and athetotic movements can be controlled by releasing them
selectively (Fig.1ABCD).
Advantages of OSSCS:
The monoarticular muscles which have antigravity activity are carefully preserved. Hence,
there is no loss of antigravity activity (muscle weakness)and no loss of sensation and
stereognosis. There is also no increase in occurrence of dislocations and deformities.
Indications are broadened:
Hypertonicity of the neck, trunk, shoulder, elbow, forearm, wrist, thumb and fingers, hip,
knee, and foot/ankle can all be controlled with the same generalized concept. All kinds of
hypertonicity (including spasticity and athetosis) are candidates for OSSCS. This control of
spasticity provides promising results for orthopaedic surgeons and also enriches the lives of people with cerebral palsy.